Authorization for Disclosure of Health Information
This file is an Authorization for Disclosure of Health Information form used for releasing health records. It enables patients to authorize the release of their medical information to designated individuals or institutions. Understanding and completing this form correctly is crucial for ensuring proper disclosure of your health information.
Edit, Download, and Sign the Authorization for Disclosure of Health Information
Form
eSign
Add Annotation
Share Form
How do I fill this out?
To fill out this form, first ensure all relevant sections are completed accurately. The patient or their representative must sign and date the form to authorize the release. Ensure to check the appropriate boxes indicating what information is to be disclosed and to whom.
How to fill out the Authorization for Disclosure of Health Information?
1
Complete all sections of the form accurately.
2
Sign and date the form where indicated.
3
Checkboxes for information disclosure must be filled out.
4
Specify the purpose of the information release.
5
Mail the completed form to the designated address.
Who needs the Authorization for Disclosure of Health Information?
1
Patients requiring access to their medical records.
2
Healthcare providers needing to share patient information.
3
Legal representatives managing patient health information.
4
Health researchers requiring anonymized patient data.
5
Family members assisting patients in managing their health information.
How PrintFriendly Works
At PrintFriendly.com, you can edit, sign, share, and download the Authorization for Disclosure of Health Information along with hundreds of thousands of other documents. Our platform helps you seamlessly edit PDFs and other documents online. You can edit our large library of pre-existing files and upload your own documents. Managing PDFs has never been easier.
Edit your Authorization for Disclosure of Health Information online.
Editing this PDF on PrintFriendly is easy and intuitive. You can update any section of the form directly in your browser, ensuring all information is accurate. Make any necessary modifications quickly and download your updated document.
Add your legally-binding signature.
You can sign the PDF on PrintFriendly directly with our easy-to-use signing feature. Just click to add your signature, ensuring all necessary authorizations are in place. This streamlined process helps you maintain compliance with health information regulations.
Share your form instantly.
Sharing your PDF from PrintFriendly is simple and fast. With just a click, you can send the document to colleagues or family members. Our sharing options ensure that your health information reaches the right people securely.
How do I edit the Authorization for Disclosure of Health Information online?
Editing this PDF on PrintFriendly is easy and intuitive. You can update any section of the form directly in your browser, ensuring all information is accurate. Make any necessary modifications quickly and download your updated document.
1
Open the PDF in PrintFriendly's editor.
2
Select the section you wish to modify.
3
Make necessary changes in the text fields.
4
Review all updates for accuracy.
5
Save your edited document and download it.

What are the instructions for submitting this form?
Please mail the completed Authorization for Disclosure of Health Information form to Thomas Jefferson University Hospitals, Inc., Health Information Management Department, 111 South 11th Street, Gibbon Building, Suite 1950, Philadelphia, PA 19107. If you have any questions regarding submission, feel free to contact our help desk for guidance. Ensure that all information is filled out correctly to avoid delays in processing.
What are the important dates for this form in 2024 and 2025?
In 2024 and 2025, it is important to note that the authorization expires six months from the date of signing unless otherwise indicated. Ensure to keep track of the dates if you plan to use this form multiple times. Review any policy changes regarding forms and disclosures annually.

What is the purpose of this form?
The purpose of the Authorization for Disclosure of Health Information form is to facilitate the legal release of a patient's medical records to designated individuals or entities. This ensures that patients' health information can be shared efficiently while complying with regulations. By using this form, patients can authorize healthcare providers to disclose their sensitive medical information as needed.
Tell me about this form and its components and fields line-by-line.
- 1. Patient Name: The full name of the patient.
- 2. Full Address: Patient's complete address including street, city, state, and zip code.
- 3. Telephone Number: Contact number for the patient.
- 4. Medical Record #: Unique identifier for patient medical records.
- 5. Date of Birth: Patient's date of birth.
- 6. Social Security Number: Partially masked social security number (last 4 digits only).
- 7. Disclosed Information: Details of the medical records and information being requested.
- 8. Purpose/Use Of The Requested Information: Kind of use for which the records are requested.
- 9. Authorization Expires: Expiration date for the authorization.
- 10. Signature: Patient's or representative's signature authorizing the request.
What happens if I fail to submit this form?
Failing to submit this form may result in an inability to access or share your health information. Healthcare providers may not be allowed to release records without proper authorization. Ensure that you complete and submit the form to avoid delays in accessing necessary information.
- Inability to Access Records: Without the completed form, you won't be able to access your medical records.
- Delays in Care: Delay in receiving care may occur if health information is not disclosed promptly.
- Legal Issues: Improper submission may lead to legal complications regarding health information sharing.
How do I know when to use this form?
- 1. Healthcare Transfers: When transferring your medical care to a new provider.
- 2. Insurance Applications: For sharing medical history with insurance companies.
- 3. Family Access: Allowing family members to access your health information.
- 4. Research Purposes: When your information is needed for health research.
- 5. Legal Proceedings: If your health records are needed for legal matters.
Frequently Asked Questions
How do I access my medical records using this form?
You can access your medical records by completing this form and submitting it to the healthcare institution.
What information do I need to disclose?
You should check all relevant boxes indicating which records or information you wish to disclose.
Can a family member sign this form for me?
Yes, a legally authorized representative can sign the form if the patient is unable.
Is there a fee for copying medical records?
Yes, there may be fees associated with copying records as regulated by state laws.
How long does it take to process this authorization?
Typically, it takes about 30 days for information maintained on-site to be processed.
Can I revoke this authorization?
Yes, you can revoke your authorization at any time by sending a written notice.
What happens if there are errors in my provided information?
Be sure to review your information carefully; incorrect or missing details could delay processing.
Where do I send the completed form?
Mail the completed form to the specified address on the document.
Can I fill out this form online?
Yes, you can complete and edit the form online using our PDF editor.
Is this form valid without a signature?
No, the form must be signed by the patient or their authorized representative to be valid.
Related Documents - Health Information Disclosure Form
Using Adventure Therapy to Assess Adlerian Lifestyle
This file explores using Adventure Therapy to assess the Adlerian lifestyle. It details Adlerian theory and traditional methods of lifestyle assessment. Includes a creative approach using Ubuntu cards.
T-Shirt Order Form for Outdoor Science School
This file contains a T-shirt order form for students attending the Outdoor Science School. It includes details on how to order shirts, pricing, and available sizes. The form also mentions scholarship shirts for bulk orders.
Mileage Log and IRS-Proof Mileage Log
This file is a comprehensive mileage log for tracking vehicle mileage. It is IRS-proof and includes fields for date, vehicle, odometer readings, mileage from start to end, etc. Essential for accurate mileage tracking.
Symbiosis National Aptitude Test 2023 Guide
This file provides important details and instructions about the Symbiosis National Aptitude Test (SNAP) 2023. It covers registration, payment deadlines, test dates, and results announcement. Additionally, it includes messages from the university's Chancellor and Pro Chancellor.

Health and Wellness Screening Instructions
This file provides comprehensive instructions for completing the health and wellness screening process. It guides users through the steps required to submit the Physician Results Form. Perfect for individuals looking to improve their health management strategies.
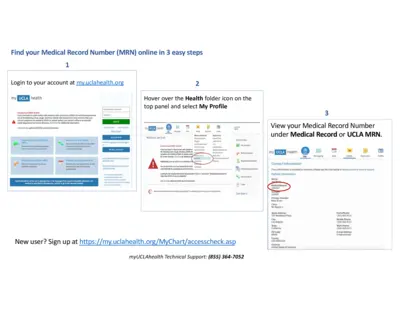
Retrieve Your Medical Record Number in 3 Steps
This file provides clear instructions for finding your Medical Record Number (MRN) online. It outlines the steps to access your MRN through the UCLA Health portal. Perfect for patients needing quick access to their medical information.
Columbus State Community College Health Record
This Health Record form is essential for documenting required Tuberculosis testing for students at Columbus State Community College. Proper completion of this form ensures compliance with public health regulations. The form includes details on testing procedures, results, and necessary follow-up actions.
Health & Wellness Life Coach Questionnaire
This file provides a detailed life coach questionnaire aimed at enhancing personal development and wellness. It includes essential questions designed to guide introspection and goal setting. Ideal for individuals seeking to improve their life satisfaction and personal growth.
2023 Wellness Wallet Reimbursement Form
The 2023 Wellness Wallet Reimbursement Form is essential for those looking to claim eligible wellness expenses. This form provides guidance on submitting claims for reimbursement related to fitness memberships, equipment purchases, and more. Ensure accuracy to avoid delays in your reimbursement claims.

Internal Call Tracking Sheet Details and Instructions
The Internal Call Tracking Sheet assists businesses in maintaining organized call records. This file allows easy tracking of customer calls for better service. Use this document to streamline your internal communication and enhance customer relations.
Patient Property and Valuables Policy Document
This file outlines the policy for the safe keeping of patient property and valuables at Doncaster and Bassetlaw Hospitals. It includes instructions for staff, legal obligations, and guidelines for handling valuables. Essential reading for all hospital staff involved in managing patients' property.
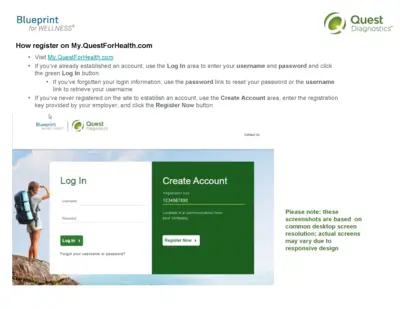
Blueprint for WELLNESS® Registration Guide
This document serves as a user-friendly guide for registering and utilizing the services on My.QuestForHealth.com. It provides step-by-step instructions and essential information to access health and wellness programs. Understand your rights and how to manage your data securely within Quest Diagnostics.

