Medicare/Medicaid Documents
Medicare/Medicaid
Medicare Part B Income-Related Premium Reduction Form
This form allows individuals who have experienced a major life-changing event that has reduced their income to request a reduction in their Medicare Part B income-related premium. It is essential for those seeking financial relief from increased premium charges. Follow the instructions carefully to ensure your application is processed promptly.
Medicare/Medicaid
Understanding Your Remittance Advice Reports
This booklet provides essential information about Remittance Advice (RA) for Medicare Providers. It helps navigate through important details regarding claim payments and adjustments. Users will find answers to common questions and guidance on using RA effectively.
Medicare/Medicaid
Medicare Power Wheelchair Coverage Overview
This document provides an overview of the coverage for power wheelchairs under Medicare. It outlines the prerequisites, patient costs, and necessary documentation required for reimbursement. Ideal for patients and healthcare providers seeking clarification on power wheelchair assistance.
Medicare/Medicaid
Medicare Coverage Drug Request Form Instructions
This document outlines the instructions for requesting a Medicare prescription drug coverage determination. It is essential for enrollees and their prescribers. Follow the guide to ensure accurate submission and prompt processing.
Medicare/Medicaid
2024 Direct Member Reimbursement Request Form
This form is for Medicare plan members to request reimbursement for dental, eyewear, and hearing aid services. It includes instructions on how to fill it out and where to send it. Ensure all required information is submitted for successful processing.
Medicare/Medicaid
Medicare Overpayments Instructions and Guidance
This file provides essential information about Medicare overpayment definitions, collection processes, and tools. Learn about payment options and the timeframe for debt collection. It serves as a comprehensive guide for beneficiaries and healthcare providers involved in Medicare financial processes.
Medicare/Medicaid
Part D Late Enrollment Penalty Reconsideration Request
This document serves as a request form for reconsidering the late enrollment penalty for Medicare Part D. It provides the necessary information and steps needed for submitting the appeal. Ensure to complete and submit this form accurately for timely processing.
Medicare/Medicaid
Medicare Beneficiary Representation Form Instructions
This file is designed to assist Medicare beneficiaries in granting authority to a representative for claims. It includes necessary information and a signature section for both the beneficiary and their representative. Follow the guidelines to ensure proper completion for liability insurance claims.
Medicare/Medicaid
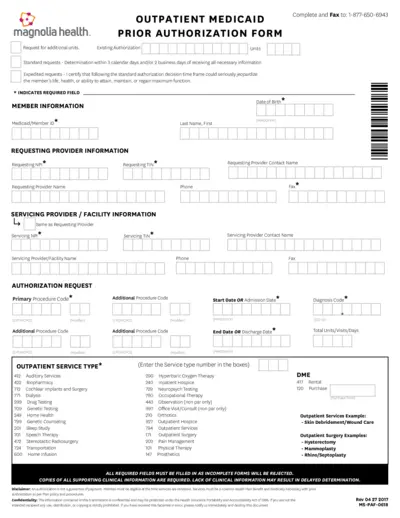
Outpatient Medicaid Prior Authorization Form
This form is essential for requesting prior authorization for Medicaid outpatient services. Filling it out correctly ensures timely processing of requests. Ensure you include all required information to avoid delays.
Medicare/Medicaid
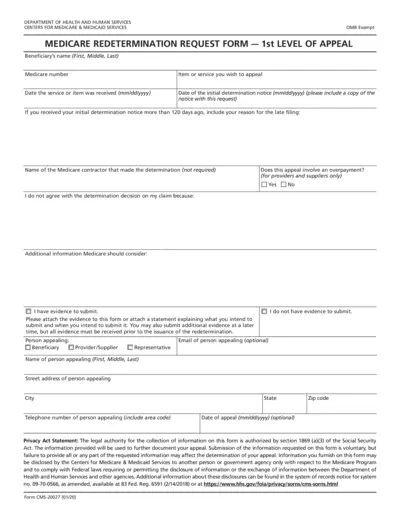
Medicare Redetermination Request Form Instructions
The Medicare Redetermination Request Form is a critical document for beneficiaries seeking to appeal Medicare decisions. This form allows users to initiate the first level of appeal for denied claims. Ensure all required information is filled accurately to expedite the review process.
Medicare/Medicaid
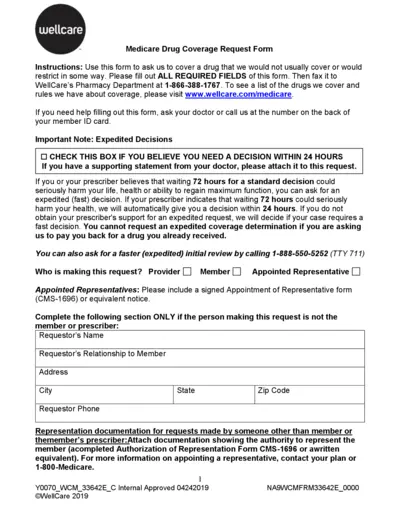
Medicare Drug Coverage Request Form
The Medicare Drug Coverage Request Form allows users to request coverage for drugs that are not typically covered. It guides members on necessary information to submit and includes important instructions for timely processing. This form is essential for members seeking medications under specific circumstances.
Medicare/Medicaid
Medicare Appeal Instructions and Rights
This document provides essential information and instructions on how to appeal Medicare service denials. It covers the rights of Medicare beneficiaries and the procedures for filing an appeal. Whether you're an individual or an advocate, this guide is invaluable for navigating Medicare's appeal process.